

BACKGROUND
Although I have not received any online comments, a technologist I work with this past Thursday told me that technologists at the regional hospital had been talking about my blogs. I was told that they have been well received. I am so happy to hear that local healthcare providers who are collaborators in community healthcare are enjoying the articles. This same capable technologist inquired about chest X-ray.
First off, I hope you Renown technologists are reading this and sharing it with your friends. Let’s delve into some basics so we all have a similar understanding, and then in future articles we will talk about the strengths and weaknesses of each technique.
THE BASICS
The chest X-ray is by far and away performed the most often by technologists and experienced by patients. In fact, it is the most common X-ray performed and remains the mainstay of thoracic imaging. Chest X-ray should always be the initial imaging study
in all patients with suspected chest/thoracic disease.
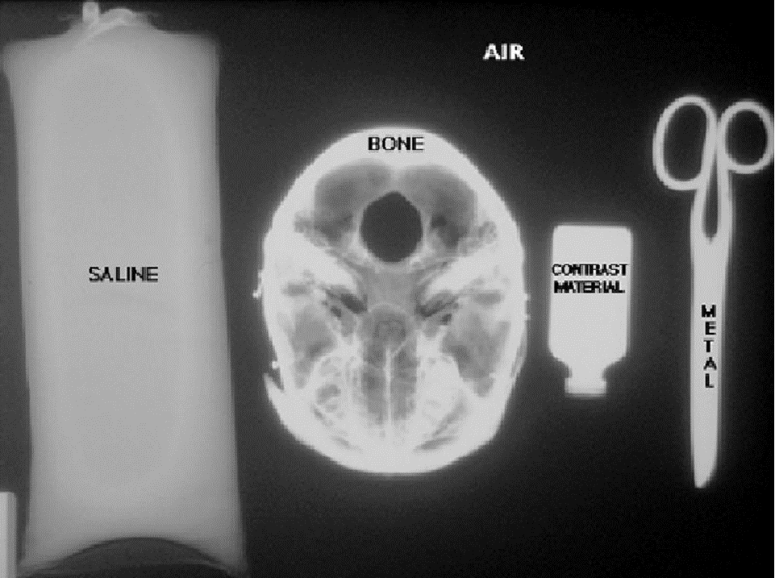
On X-ray the density of an object is related to the structures ability to block photons/X-rays. Air allows all the photons to pass exposing more film and generating a black image. More dense structures, such as bone or metal, reflect or absorb photons and the film appears white.
There are ordering options available to clinicians for chest X-rays. The gold standard would be the PA and lateral view, but often not necessary. The AP portable view of the chest is the most common in the ICU and ER. Then there are specialty views like the decubitus, apical lordotic, and expiratory views, each of which should be utilized in the appropriate clinical setting.
COMMON TECHNIQUES
PA View: The patient’s chest is placed against the film cassette. X-rays enter the patient posteriorly/in the back (P) and exit anteriorly/out the chest (A). This technique provides the most accurate anatomic correlate with the patient’s body. Here the heart is closest to the film/image collector making the heart appear about the correct size. The lungs should be well-expanded with the patient taking a good to great effort at taking in and holding a reasonable sized breath. Too little and the lungs can appear congested and too much may hint at COPD. Patients just please follow your kind technologists instructions. This is often done with a lateral projection for a total of two views.

Lateral View: Taken from the side with the patients arms up.

AP View: Performed on patients who are unable to stand or maybe weak or unsteady on their feet. This exam is often done at the bedside with the film cassette placed directly under the patient’s back. Here the xrays enter the chest anteriorly and exit posteriorly. This causes the heart to appear larger than it actually is. Do it yourself. Fist close to a wall with a flashlight on about 1-2 feet away (that’s PA). Bring your fist closer to the light and notice how it appears larger (that’s AP). Your fist is obviously our example of the size of your heart and wrist being the central chest structures.

Let’s break here and get into chest X-ray anatomy next time. I hope this provided help to someone out there. I feel like it is the first act and we are just setting the stage for the excitement to come. After anatomy we will tackle some common chest X-ray pathology. I was specifically asked to tackle appropriate views for differing clinical situations (e.g. ER, outpatient, ICU, inpatient) and we will see where this series leads.
Hey, someone from Renown Regional Medical Center in Reno, NV, I’m calling you out. Please say hi to me. I’m a nice, friendly guy. I promise.
Thanks,
Ron

Great article!
LikeLike
I’m glad you liked it. I hope you enjoy the series. More to come so stay tuned.
Thanks,
Ron
LikeLike
Dr. Swanger, I am a technologist at Renown Regional. THANK YOU for this blog! I have tried submitting comments a few times before, but they never seemed to post (apparently wordpress doesn’t like my iPhone?). Your blog is an incredible resource to gain insight into a Rad’s perspective. Not only does this make me a better technologist in terms of image quality, but it provides useful, relatable knowledge that allows me to better educate and communicate with patients, students, and other Allied Health professionals. Thank you especially for your mammo series! I know that it’s boring to most, but I am beginning cross-training, and the research I have found online has been meager and out-dated. Keep on blogging, Sir!
LikeLike
Hi Annikki,
Thank you SO MUCH for your comment! It is great to know I am reaching people, and that they are local is wonderful. I sure hope we get a chance to meet sometime. Your feedback is very motivating. I’m so happy that I can provide some help and benefit to you and others ultimately to the help and health of our patients. I’ll keep blogging if you keep reading… and commenting occasionally so I know you are reading.
Thanks,
Ron
LikeLike
My pleasure! I am quite confident we will meet at some point. The local medical imaging community is small, and I am good friends with three of your techs at RDC (Dawn, Susan, and Clarissa)! I will absolutely keep reading, sharing it with others, and commenting from time to time. Thanks again!
LikeLike
I want more more more! You provide wonderfully educational and well-written articles. Patients want the mystery taken out of our bodies and our medical information. We want to be engaged in our health care management. Physicians like you (far too rare) are delightfully refreshing with your compassion and straight forwardness to help us learn and address what is best for us. Thank you.
LikeLike
Thank you so much for the encouragement. I’ll do my best to please!!!
LikeLike